|
|
The Minimal Cleft |
|
|---|

|
|
|
The obsolete straight line repair (Fig.14) is potentially the most destructive of all lip repairs. Early surgeons, unaware of tissue malposition, thought that cleft lips had a tissue deficiency causing the lip to be too short on the cleft side. Based on this misdiagnosis, they used curved excisions of lip tissue (Fig.14B) out far enough on each side of the cleft, such that, when closed in a straight line (Fig.14C), the lip length would be increased. This operation throws away important lip anatomy simply in order to fill a gap; nothing else is corrected. All remaining lip tissue is left in the abnormal cleft position. Fig.14D is a clinical example in which the result of a straight line repair can be easily related to the artist's rendition in Fig.14C. Note the remaining philtral remnant in its original malrotated position. |
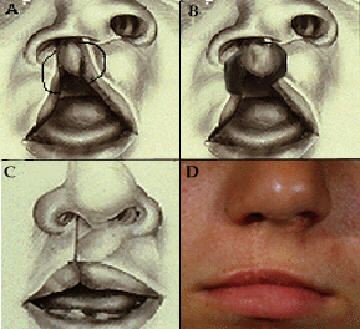
Fig. 14 |
|
Fig.15 shows four more examples of lips repaired with the straight line technique. Depending on how much tissue is discarded, results vary from the appearance of a simple lip adhesion (Fig.15A), wherein only the vermilion edges were excised, to tight lips devoid of normal anatomic landmarks (Fig.15C and D), when large amounts of lip were removed. But why even mention this outdated repair? Even today, one occasionally sees the unsatisfactory result of a surgeon who determined that a cleft was so mild that he/she decided to use a straight line repair. |
|
Fig. 15 |
|
Fig.16A shows an example of such a case. Whenever there is any philtral malrotation, a straight line repair requires excision of a small portion of the philtrum to permit white roll alignment. Fig. 16B, in which the points of cupid's bow are highlighted, shows the extent of missing philtral tissue. |
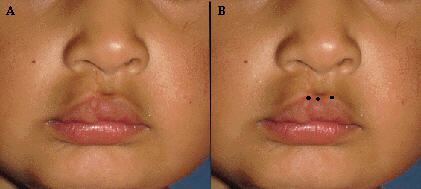
Fig. 16 |
|
Fig. 17 is a computer generated demonstration of the etiology of this deformity: Fig. 17A - A mild, incomplete cleft with a very small amount of malrotation. Fig. 17B - The location of the high point mark, on the cleft side of the philtrum, to allow it to align with its mate on the white roll of the lateral lip. Fig. 17C - Incisions are designed, thus showing how much tissue would have to be discarded, to excise enough tissue to permit the white roll of medial and lateral elements to be approximated. Fig. 17D - The resultant deformity, created on the computer, reproduced the obvious asymmetry of cupid's bow seen in Fig.16A. It is true that Millard reported one case wherein he closed a mild cleft with a straight line technique2 (p 304). In so doing, however, he stressed two important points: there was no philtral malrotation, and the lip could be repaired without excising any philtral tissue! The main surgical principle for a good lip repair remains that of returning displaced, but otherwise normal, tissue to normal position. If there is any malrotation of the unit, a R-A repair is indicated. |
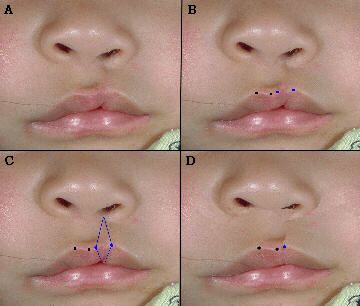
Fig. 17 |
|
Fig.18A shows such a case; Fig.18B is the post-op result of the R-A repair. When comparing Fig. 18B to Fig.16A, one can easily conclude that straight line repairs are contraindicated and the R-A repair is the procedure of choice for minimal clefts. |

Fig. 18 |
|
|
