|
|
Marking the Advancement Flaps |
|
|---|

|
|
|
The precise determination of the high point of cupid's bow on the lateral lip element is another critical procedure for an excellent lip repair. Mistakes in properly identifying this point are not unique to any specific repair. Fig. 35, with the surgical scar highlighted on the left, demonstrates a poorly done triangular flap repair in which the surgeon placed the high point too far up in the cleft, leaving too much white roll and vermilion in the lateral element. This resulted in a vermilion mismatch as well as excessive bulk in the lateral element. |

Fig. 35 |
|
Fig. 36B shows the same deformity in a R-A repair. By comparing the pre- and post-op views, one can easily see where the surgeon had approximated the lip elements, retaining far too much lateral element vermilion in the advancement flap. Why did that happen? Some surgeons use an unreliable rule of thumb: locate the high point "where the white roll disappears." In this case, careful inspection of the pre-op photo shows a white roll extending far up the lateral element. |

Fig. 36 |
|
Fig. 37A shows the approximate location where the surgeon marked the high point in this case; Fig. 37B shows where it should have been. |
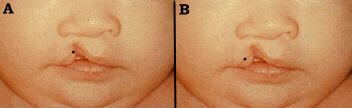
Fig. 37 |
|
Fig. 38 is another, less overt, example of the same phenomenon; note the excess fullness and abnormal curvature of the lateral element vermilion. The proper lateral lip high point usually does not correlate with white roll disappearance. "Where the white roll disappears" is an "old surgeon's tale" that can be very misleading. |

Fig. 38 |
|
The opposite problem is demonstrated in Fig. 39, another patient who had a poorly done R-A repair. In this case, the surgeon came too far out on the lateral element and, as a result, threw away an alarming amount of normal lip tissue. This result is reminiscent of the most destructive straight line or Mirault repairs of old. How could this happen? |

Fig. 39 |
|
By measuring the alar base-to-high point distance on the normal, non-cleft side and rigidly applying it to the shortened, cleft side while marking. In many cases these measurements compare favorably. But, in some complete clefts, especially those with an apparent lateral element deficiency, this ill advised practice will cause one to come too far out on the lateral element. Do not think numbers; think anatomy! How about using the normal side commissure-to-high-point measurement and applying it to the cleft side? Once again, in many lips this will work. However, in the more severe clefts, especially complete clefts, the distance from the oral commissure to the high point is shorter on the cleft side. This is due to the lack of lip continuity keeping the lateral element muscle from assuming its normal stretched position. Gently stretching the lateral lip element reveals its potential dimensions; but how does an inexperienced surgeon know if he/she is pulling too hard, or hard enough, to establish the proper location of the high point?
The following is presented as a reliable technique for determining the lateral side high point. Similar to the marking the philtral unit, the lateral lip must be marked while looking at its unique perspective (Fig.40). While looking at the lateral lip element, from the side, locate the highest point on the dome of the white roll; not the vermilion, the white roll. This is the location of the lateral element high point. The tissue above this point belongs in the lip; that below, in the vermilion. Using the top of this dome to determine the high point has proven to be a valuable,consistently precise, anatomic guideline in marking the lateral element. |
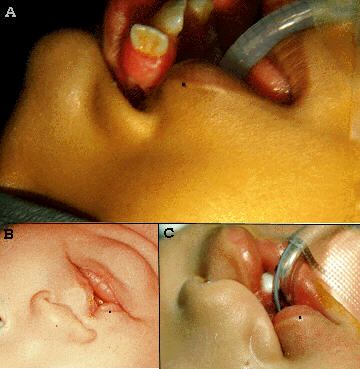
Fig. 40 |
|
Fig. 41 demonstrates the use of this technique. |

Fig. 41 |
|
Fig. 42 shows four examples of completely marked advancement flaps. After connecting the high point to the alar crease, at the appropriate length, the marking continues in the crease around the alar base. Rarely, one must use a small amount of skin from the alar base to achieve adequate length in the advancement flap. One is able to identify which lips are candidates for this modification after determining the ideal location of the high point. Lastly, when drawing the the advancement flap, it is imperative that one does not leave any white roll or vermilion on the edge of the advancement flap. |
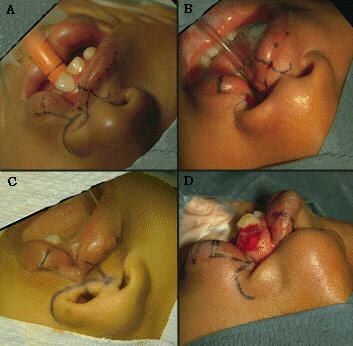
Fig. 42 |
|
The presence of white roll or vermilion in the rotation scar renders the scar unsightly (Fig.43), acting like a beacon in calling attention to itself. |
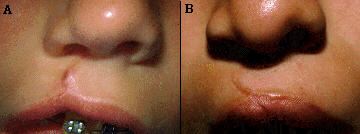
Fig. 43 |
|
|