|
|
The Vermilion Cuts (Is this an important issue? ) |
|
|---|

|
|
|
Why does the lip in Fig. 44, which had a triangular flap repair, seem so unnatural? Part of the tubercle is missing because a small amount of the philtral vermilion was inadvertently discarded. This notching, or whistling deformity, of the free vermilion edge was also a result of an error in marking; the error was also made because the surgeon failed to appreciate the full extent of the anatomic unit. |

Fig. 44 |
|
For maximal preservation, vermilion cuts must be made at least perpendicular to the white roll to preserve proper balance (Fig. 45A). If , when marking the rotation cut, one continues straight into the tubercle vermilion (Fig. 45B) rather than making the cut at 90 degrees to the white roll, important tissue will be lost. |
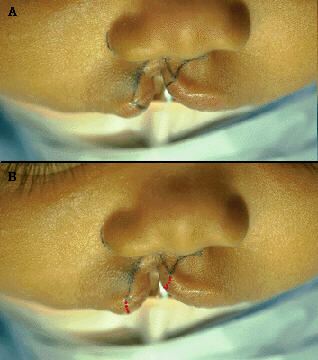
Fig. 45 |
|
Mismarking the vermilion as shown in Fig. 46A (red line) will result in the kind of philtral tubercle deformity exhibited in Fig. 46B. |
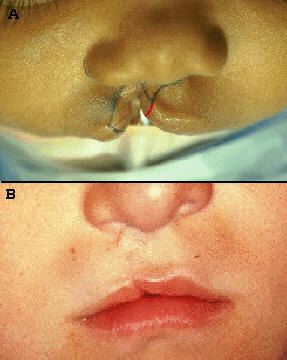
Fig. 46 |
|
Similarly, if one continues the vermilion cut obliquely out on the lateral element vermilion, as depicted in Fig. 47A, too much vermilion will be discarded. The result? Noticeable lip asymmetry with a flattened, deficient lateral vermilion, as depicted in a different patient in Fig. 47B. Fig. 45A shows the correct way to mark the vermilion cuts: Where the rotation and advancement cuts meets the white roll, the vermilion continuation of this cut must be made at least perpendicular to the white roll. This will insure that all vermilion belonging to the tubercle and the lateral lip will be preserved. |
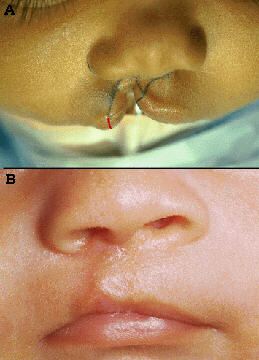
Fig. 47 |
|
Fig. 48 shows the lateral and medial lip markings on two patients which demonstrate the vermilion cuts at a 90 degree angle to the white roll. Will this always be enough? No. Some cleft lips require more. One must compare the vermilion bulk of the medial and lateral elements at their respective cleft high points of cupid's bow. When there is significant discrepancy in vermilion bulk, extra vermilion should be preserved on the fuller side, sometimes on both sides. |
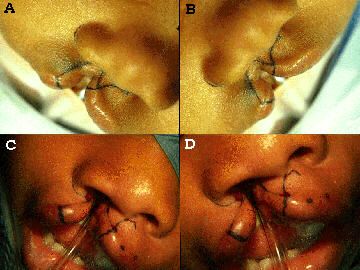
Fig. 48 |
|
In Fig. 49, instead of a perpendicular cut, the pre-op marking shows extra lateral element vermilion being preserved for later augmentation of the deficient medial element. The post-op view demonstrates that tissue being used as a transposition flap hidden under the tubercle vermilion. This flap added the necessary fullness for the normal protrusion of the unit. One must always anticipate the need for this variation when marking the lip. |

Fig. 49 |
|
|