|
|
Muscle Alignment |
|
|---|

|
|
|
A cleft lip closed without correcting the abnormal muscle anatomy of the advancement flap will produce two distinct deformities: 1. A characteristic muscle bulge in the lateral element (Fig.54A,B). This deformity is seen more often in the more severe clefts. The foreshortened lateral lip muscle remains "in situ", inserted into the alar base, rather than having been freed up and properly oriented to the rotation flap. 2. A marked depression at the tip of the advancement flap (Fig. 54C and D). This problem, also most often seen in the more severe clefts, is due to inadequate muscle bulk beneath the tip of the advancement flap. This is occasionally seen even in recent papers concerning cleft lip repair1. |

Fig. 54 |
|
Some have recommended that the rotation flap cut-back be continued until the philtrum can be "gently" pulled into correct position (Fig.51). How much pull is enough? How much pull is too much? |
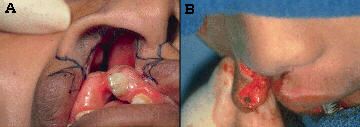
Fig. 55 |
|
If the lateral flap is simply advanced without correcting this problem (Fig.56A,B), the noticeable depression in the advancement flap tip (Fig.56C,D) will ensue. |
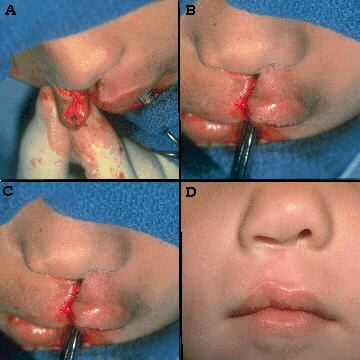
Fig. 56 |
|
Preventing these deformities is straightforward: 1. Continue the cut in the alar base crease far enough to completely separate the advancement flap, and its muscle, from their attachments to the alar base (Fig.57A). 2. Dissect the skin away from the underlying muscle enough to allow the muscle to be advanced independent from the skin (Fig.57B). |
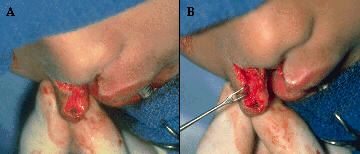
Fig. 57 |
|
3. Find the point at which, when pulling on (advancing) the upper edge of the muscle (Fig.58A,C), one's forceps come to lie directly under the tip of the skin flap (Fig.58B,D). This is the proper location for the suture to be placed in the muscle of the lateral element to advance it into the apex of the rotation flap. This muscle advancement provides a full bodied muscle platform upon which the skin tip of the advancement flap will rest. Because the lateral lip muscle is detached from the nasal alar base, repositioned, and appropriately stretched, the unsightly bulge shown in Fig. 54, A and B, is avoided. |
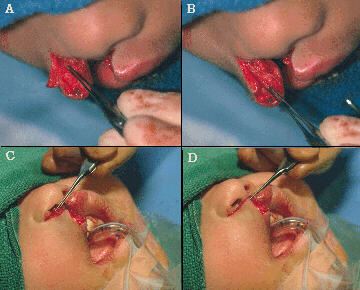
Fig. 58 |
|
Fig. 59A shows the appearance of the repair after the muscle has been advanced into the rotation defect. Fig. 59B shows the skin tip of the advancement flap sitting on this solid muscle platform, giving the lip a normal anatomic fullness and balance. |
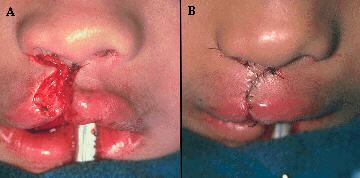
Fig. 59 |
|
|