|
|
The Rotation Cuts (How much cutback is enough?) |
|
|---|

|
|
|
The details of the rotating the philtrum, including the importance of deep muscle release as the dissection continues, are clearly outlined by Millard2, 10. One occasionally sees examples of under rotation (Fig.50A,B,C) or over rotation (Fig.50D). Over rotation will occur if one keeps cutting back on the rotation flap until the philtrum simply "lies", unassisted, in horizontal position. Adequate rotation will have been achieved long before that point. Normal soft tissue "memory" in the tissue remaining attached to the philtrum, even after adequate release, inhibits the philtrum from simply lying in place; if one continues the cut-back until it does so, one has gone too far. |
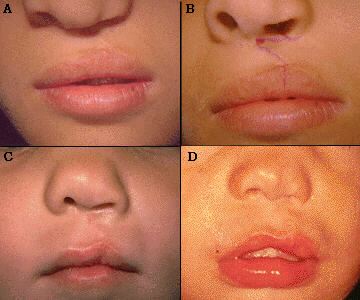
Fig. 50 |
|
Some have recommended that the rotation flap cut-back be continued until the philtrum can be "gently" pulled into correct position (Fig.51). How much pull is enough? How much pull is too much? |

Fig. 51 |
|
The following technique has proven reliable in determining adequate philtral release (Fig.52): 1. Apply digital pressure to both alar bases, firmly enough to push them together (pushing the alar bases together does not put any pressure on the philtrum, but it does allow the philtrum to swing freely on its own axis) 2. Note the position of the philtrum. An adequately released philtrum, pivoting only on its remaining attachment to the lateral lip, will easily assume a horizontal position (Fig.52B). |
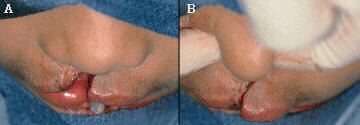
Fig. 52 |
|
3. When there is prominent premaxillary protrusion, pressing the non-cleft alar base against the premaxilla will accomplish the same thing (Fig.53). So, continue the rotation release and/or cut-back until, when firmly pressing the alar bases together, the philtral unit, on its own axis, easily swings into proper horizontal position. |
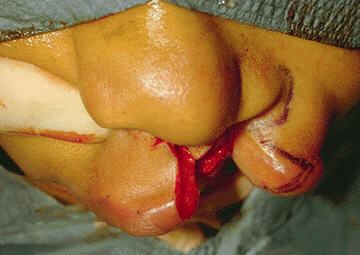
Fig. 53 |
|
|