|
|
Triangular Flap Repairs |
|
|---|

|
|
|
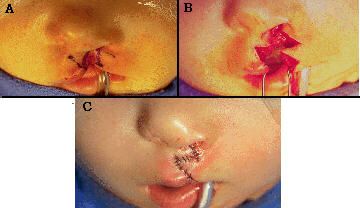
In 1952, Tennison4 described his "stencil" method of cleft lip repair which preserved cupid's bow, thus beginning the "Z", or triangle flap, era in cleft lip repairs. Basically, two methods of triangular flap repairs have evolved: the "rotation-transposition" procedure (e.g., Tennison4 and Randall6) and the true "Z"-plasty (e.g., Marcks1 and Davies7). Fig.5 demonstrates the
"rotation-transposition" procedure.
|
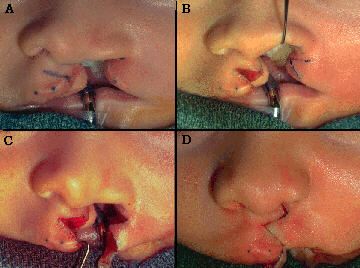
Fig. 5 |
|
Fig.6 illustrates the "Z"-plasty principle, as advocated by Davies7,which gets to the same place, with similar tissue, but in a different way: using double transposition flaps instead of rotation-transposition flaps. Fig.6A - Sixty degree equilateral triangle flaps are designed such that the length of each limb is equal to 4/7 of the height of the lip (alar base to high point) on the normal side. Fig.6B - These flaps are mutually transposed, gaining a theoretic 75% increase in length along the axis of the "Z" (this is where the 4/7ths came from!). Fig.6C - Cupid's bow, more or less going along for the ride, ends up in the horizontal position when the lengthening measurements are geometrically accurate.
|
|
Fig. 6 |
|
Fig.7 displays, side by side, the tissue "motion" shown in Fig.5C and that in Fig.6B. When comparing these views, one immediately sees the similarity of the rotation-transposition and the "Z"-plasty techniques. The differences are more in concept than execution. |
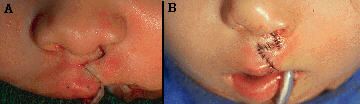
Fig. 7 |
|
Fig.8 shows four cases demonstrating a well-known risk for all triangular flap lip repairs: an abnormally long lip on the cleft side. Why does this happen? The lateral element transposition flap uses tissue that, with growth, increases upper lip width. After this tissue is transposed, its growth orientation is changed from horizontal to vertical. Therefore, a perfectly balanced lip at the time of repair may become too long as the patient grows older.
|
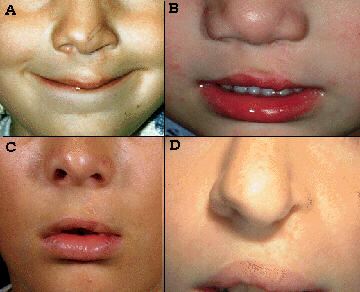
Fig. 8 |
|
The main argument against triangle lip repairs is a "Z" shaped scar located where one would expect to see a curvilinear philtral column (Fig.9). Even in well-balanced lips, the lateral transposition flaps in triangle repairs can be seen "invading" the philtral unit. A small flap situated low in the philtrum (e.g., Fig.9D) is more obvious than a larger flap placed higher in the philtrum (e.g., Fig.9C). In all cases, however, "Z" repairs fail to establish philtral symmetry. Those using triangular flap repairs have no hope of, and give no consideration to, leaving a scar that imitates a normal philtral column. |
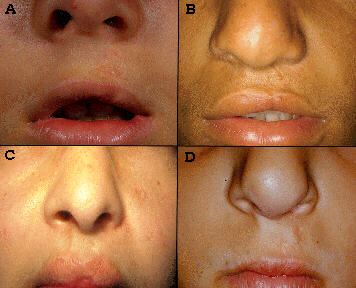
Fig. 9 |
|
|